Types of Cancer Immunotherapy
Monoclonal Antibodies (mABs): Ex vivo, created antibodies that target a specific antigen (protein) on the surface of the cancer cell, “marking” that cell to be destroyed by the immune system. These medications may also work by blocking a “receptor” found on cells that is important to growth. This type of immune therapy drugs, such as, rituximab (Rituxan®), bevacizumab (Avastin®), trastuzumab (Herceptin®), and denosumab (Xgeva®, Prolia®).
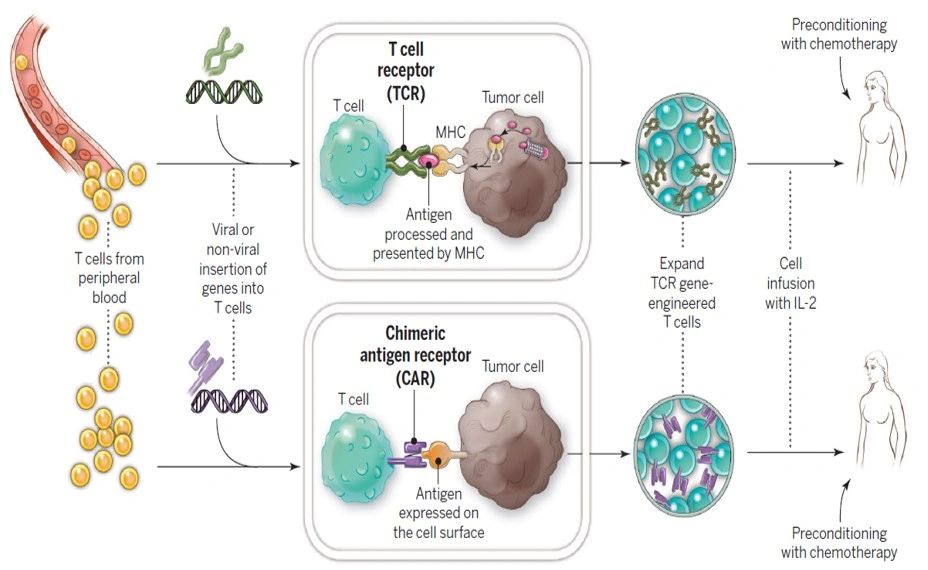
Adoptive T-Cell Transfer: This type of immune therapy encourages the bodies T-cells to fight cancer. There are two types of this treatment. The first removes T-cells directly from a patient’s tumor, produces large quantities of these cells outside the body and then re-infuses them back to the patient. The second method also removes T-cells from the patient, but the cells are then enhanced in the lab with new receptors, called chimeric antigen receptors (CAR-T). These receptors target specific antigens in the patient’s cancer cells, stimulating the immune response against the cancer. Examples of CAR-T treatments include tisagenlecleucel and axicabtagene ciloleucel.
Donor Lymphocyte Therapy (DLI): DLI involves the infusion of lymphocytes (type of white blood cell) from a donor to a patient who has already had an allogenic bone marrow transplant from the same donor. The donor lymphocytes may assist in identifying targets for immune system attack. This can induce remission or potentially prevent relapse in patients who are at high risk for relapse after bone marrow transplant. DLI can also cause graft versus host disease (GVHD), a potentially serious side effect in which the recipient’s cells/tissues are attacked by the donor immune cells.
T Cell or NK Cell Engaging Bispecific Antibody (T-BsAb)
Monoclonal antibodies engage the innate immune system to destroy targeted cells. For the last 30years, antibody-dependent cell-mediated cytotoxicity and complement-dependent cytotoxicity have been the main mechanisms of anti-tumor action of unconjugated antibody drugs. Efforts to exploit the potentials of other immune cells, in particular T cells, culminated in the recent approval of two T cell engaging bispecific antibody (T-BsAb) drugs, thereby stimulating new efforts to accelerate similar platforms through preclinical and clinical trials. In this review, we have compiled the worldwide effort in exploring T cell engaging bispecific antibodies. Our special emphasis is on the lessons learned, with the hope to derive insights in this fast evolving field with tremendous clinical potential.
Cancer Vaccines: Like other vaccines, cancer vaccines are comprised of cells that have been modified in vitro to direct an immune response. There are a few different types of cancer vaccines, but primarily they function either to prevent disease (example: the HPV vaccine) or to treat the cancer directly (tumor cell vaccines, antigen vaccines, dendritic cell vaccines or vector-based vaccines).
Cytokine Therapies: Cytokines play a very specific role in the immune system. They facilitate communication among different immune cells, while also assisting in the launch of an immune response. When cytokine therapy is used to fight cancer, it is focused on using the substances to promote immune system response. Examples of cytokines include interferon, interleukin (IL-2 etc), and colony stimulating factors (Leukine®, GM-CSF).
Immune Checkpoint Inhibitors: These medications block tumor cells from inactivating T cells. This allows the T cell (and the immune system) to remain active in fighting the tumor. Examples of immune checkpoint inhibitors include: ipilimumab (Yervoy®), nivolumab (Opdivo®) and pembrolizumab (Keytruda®).
Radioimmunotherapy: This is a combination of a monoclonal antibody and a radiation source. This results in radiation being delivered directly to the specific tumor cells, but often in lower doses and over a longer period of time. An example is ibritumomab tiuxetan (Zevalin®).
Virus Immunotherapy: This type of therapy uses viruses to deliberately infect the cancer cells, which then triggers an immune system response against the virus (and the virus infected cancer cells). Examples of viruses being used to study this therapy include the polio virus and the herpes simplex virus. These methods are still being studied in clinical trials.